Exogenous intervention in mRNA transcription
BSRA 2024 Poster - aka "I ate a lot of citrate"
This contains the details of the Poster being displayed at BSRA2024 in Birmingham. Unlike the poster it also includes links to papers which are implicitly referred to in the poster itself.
Abstract
In an N=1 biohacking experiment without randomisation or placebo control in a white man in his 60s, the use of a combination of daily citrate supplementation (varying numbers of grams between 2 and 70) and histone deacetylase inhibition was found to reduce the background level of C Reactive Protein consistent with a reduction in the burden of senescent cells, encourage new hair growth and the repigmentation of hair on a dose dependent basis, enable more rapid repair of a venepuncture insult, enable easier muscle growth and improve metabolic balance. This was consistent with improving the transcription of mRNA so that the longer genes which often have difficulty being transcribed during aging were transcribed.
Other individuals have experimented with a similar protocol with anecdotal reports of similar improvements and further research is warranted.
References
References to the publications used in this poster can be found at the URL https://citrate.science/2024poster/poster.html
Introduction
There are a number of different hypotheses as to why the hallmarks of aging occur. One hypothesis is that as cells age the genome has difficulties producing longer genes. Some papers point to this arising from a shortage of nuclear acetyl-CoA. This has been seen for osteoporosis to be caused by low expression of the mitochondrial citrate carrier (SLC25A1).
The link between nuclear acetyl-CoA levels and the splicing of mRNA is well known.
The author wondered to what extent this was more broadly caused by a mixture of a shortage of expression of SLC25A1, but also by a reduction in mitochondrial membrane potential resulting in a lower efflux of citrate via the Citrate Carrier. (The Genomic Failure Hypothesis)
The author therefore decided to experiment with attempting to systemically adjust the process of mRNA translation for himself by a combination of interventions aiming to encourage the transcription of longer genes and particularly the splices that occur with higher energy availability.
Aging is associated with a systemic length-associated transcriptome imbalance
Age- or lifestyle-induced accumulation of genotoxicity is associated with a generalized shutdown of long gene transcription and
Gene Size Matters: An Analysis of Gene Length in the Human Genome
Human aging is characterized by focused changes in gene expression and deregulation of alternative splicing
Genome-wide RNA polymerase stalling shapes the transcriptome during aging
Chromatin remodeling due to degradation of citrate carrier impairs osteogenesis of aged mesenchymal stem cells
Edit 9/11/24 I just found this paper which points to the power constraints on differentiation (much like the osteoporosis issue)
Differentiation reveals latent features of aging and an energy barrier in murine myogenesis
Eusocial Hymenoptera (Queen Bee/Ant)
It is well known that the queens of bees and ants have a different phenotype. This is material because they also live considerably longer than worker bees which otherwise have the same genes. This has been studied in some detail in bees and it is known that the substance Royal Jelly which is eaten by Queen Bees for all of their life (but by worker bees for only 3 days) has the effect of changing the phenotype to a queen.
Royal Jelly contains a weak HDAC inhibitor, a Coenzyme A precursor (Vitamin B5) and AMPK activators. Hence it would be expected to enhance mRNA transcription.
Queen termites also have a changed phenotype, but the literature is not as clear as to the reasons for this.
The use of Drosophila melanogaster as a screening agent for longevity factors; pantothenic acid as a longevity factor in royal jelly
Histone deacetylase inhibitor activity in royal jelly might facilitate caste switching in bees
New Insights into the Biological and Pharmaceutical Properties of Royal Jelly
Disentangling the aging gene expression network of termite queens
Extended longevity of termite kings and queens is accompanied by extranuclear localization of telomerase in somatic organs and caste-specific expression of its isoforms note link to splicing variants
Royal Jelly for Homo Sapiens and XPRIZE Healthspan
In essence, therefore, a mixture of citrate, various natural HDAC inihibitors and other supplements are being used as an equivalent of Royal Jelly, but for Human Beings.
This is the basis for a protocol for the "Biohacking to Improve Everyone's Health" team which has been entered for XPRIZE Healthspan.
Splicing variations and Acetyl-Coa dynamics
The flow of acetyl-CoA in the cytosol and nucleus is quite complex. The main two sources are from citrate conversion with ACLY and acetate conversion with ACSS2. However, acetyl-CoA can then be used for a number of purposes of which only one is acetylation of the histone. However, from a signalling perspective it can be seen that levels of acetyl-CoA are indicative of the power (measured in Watts) available from the mitochondria. Hence if acetyl-CoA levels are higher then genes which require more power can be produced.
The balance in energy usage between transcription and translation can be controlled, therefore, by the power availability in the cell. The balance between splicing variations for any one gene will be driven at least in part by the level of power available in the cell. If a gene is not transcribed in whatever splicing format then it will not call on ATP resources for translation.
Where splicing joins chromatin
Questions about mRNA transcription
mRNA transcription has had considerable attention over the years. It is accepted that for the process of transcription to occur that the histone requires acetylation. This requires the Histone Acetylation Transferase that travels with the RNA Polymerase II complex to have acetyl-CoA as a substrate. More recently research has pointed to difficulties with RNA Pol II being stalled. Research has also pointed to Histone Deacetylases impacting on transcription. The authors search of the literature has not identified any conclusive explanation as to the mechanism for this. The author wonders whether it may involve the deacetylation of the histone close to the point at which RNA Pol II is stalled. This could involve deacetylation of the histone just prior to where RNA Poll II is stalled so if RNA Pol II goes into reverse it encounters a termination position.
Suffice to say that there is evidence that some hyperacetylation leads to ATP depletion and atoptosis. There is also considerable evidence that HDAC inhibitors of whatever class do impact on transcription as do HDAC's themselves.
From a practical perspective, therefore, there is a good mechanistic hypothesis for making use of HDAC inhibitors as part of a package of interventions to interfere, hopefully in a positive manner, with transcription.
Histone deacetylase inhibitors induce apoptosis, histone hyperacetylation and up-regulation of gene transcription in Schistosoma mansoni
Natural HDAC inhibitors
There are a number of well known herbal substances that have been used medically for many years. A quartet involving curcumin, quercetin, pterostilbene and berberine were selected as the first intervention quartet. However, other HDAC inhibitors have been tested as well although none of the results of those experiments are reported here. The first quartet were selected because as natural compounds that have been used for a long period of time their safety record is clear. They tend to operate with an IC50 in the 10s of micromolar range.
Role of histone acetylation in gastric cancer: implications of dietetic compounds and clinical perspectives
Mitochondrial Heteroplasmy, the MMP, AMPK and Traditional Chinese Medicine
The Mitochondrial Membrane Potential and rate of citrate efflux appear to be quite closely linked.
This is clearly from an evolutionary perspective the signalling mechanism that acetylation is relying on. Hence as mtDNA gets damaged and heteroplasmy increases with often associated damage to the electron transport chain then the level of citrate efflux reduces. Obviously another mechanism for improving this (and probably a better one, but harder to do) is to improve the mitochondrial quality. This is probably the primary pathway through which damage causes an aging effect whereas the secondary is through the accumulation of senescence.
There are a number of tools including mitophagy, for which the use of Rapamycin is helpful and other similar mechnisms. Also activating AMPK is useful.
Within TCM there is a category of herbs known as Yang Qi activators. Looking at the literature these seem to be almost entirely AMPK activators. As part of the protocol some experimentation has been done with these without any conclusive result as yet although this will form part of the XPRIZE Healthspan protocol.
Yang/Qi Invigoration: An Herbal Therapy for Chronic Fatigue Syndrome with Yang Deficiency?
Citrate Flows - The ins and outs of citrate
There is clearly a question as to what extent citrate gets into cells other than liver cells. Apart from the citrate carrier that takes citrate from the mitochondria there are a number of carriers in the cell membrane itself. The main three are SLC13A2, SLC13A3 and SLC13A5 (also known as INDY in Drosophila or mINDY in Homo Sapiens). These vary in their expression in different cells, but a small amount of expression is seen in a number of cells. Additionally there is a splicing variant of the mitochondrial citrate carrier that places the protein in the cell wall rather than the inner mitochondrial membrane. This has the interesting potential effect that as acetyl-CoA levels go down in the cytosol a protein is expressed that extracts citrate from serum, if it is there.
SLC13A5 is strongly expressed in liver cells and acts to draw citrate from serum. This gives rise to citrate's 30 minute serum half life. However, there is evidence for a low level of citrate transport in other tissues.
Citrate, a Ubiquitous Key Metabolite with Regulatory Function in the CNS
Mitochondrial and Plasma Membrane Citrate Transporters: Discovery of Selective Inhibitors and Application to Structure/Function Analysis
Permeability of human and rat red blood cells to citrate
SLC13A2 expression
SLC13A3 expression
SLC13A5 expression
SLC25A1 expression - the mitochondrial citrate carrier
Specificially looking at the pmCIC
Molecular origin of plasma membrane citrate transporter in human prostate epithelial cells
Extracellular Citrate Affects Critical Elements of Cancer Cell Metabolism and Supports Cancer Development In Vivo
Additional commentary: These show that the splicing variants of SLC25A1 that place it in the cell membrane can result in the citrate/malate antiporter working in both directions. However, the key point is that a splicing variant can operate where power levels are lower to import extracellular citrate.
Citrate and Cancer
There have been suggestions that citrate could be used to treat cancer. There have been a number of reviews written about this and also higher serum citrate is not always a sign of better health, sometimes it is a sign of worse health. The references for this are on the citrate.science website.
Targeting citrate as a novel therapeutic strategy in cancer treatment
The dual role of citrate in cancer
Prostate Cancer and BPH
The prostate is an interesting organ from the perspective of epigenetics in that it acts to place citrate in the seminal fluid. That has the evolutionary advantage of making it possible for the zygote to take some citrate from the external environment to assist with acetylation of the histone at the point at which rapid division is occurring.
Prostate cancer is also associated with serum citrate levels in that lower serum citrate levels point to a prostate cancer diagnosis.
Prostate cancer itself is strongly associated with aberrant splicing. It is, therefore, possible that exogenous citrate could reduce the amount of aberrant splicing. The only tests results are the usual N=1 test results from one individual, but that does give a value for PSA which in most cases below 1 microgram per litre. This varies negatively associated with citrate supplementation levels.
Concepts of citrate production and secretion by prostate 1. Metabolic relationships
Prostate Cancer: Alternatively Spliced mRNA Transcripts in Tumor Progression and Their Uses as Therapeutic Targets
Glucose handling
Acetylation is required for the transcription of non-coding DNA as well as coding DNA. The results from CGM were used both prior to starting the citrate protocol as well as having been doing it for a year. This pointed to an improvement in glucose handling such that the peak following a standardised breakfast (beans, bacon, sausage, toast and tea) reduced from 10mmol/L to 8mmol/L. This pointed to glucose handling being improved such that the polyol pathway was not activated.
The test subjects HbA1c remained below 5%. (The minimum was 4.18%).

Biochemistry, Polyol Or Sorbitol Pathways
C Reactive Protein. (CRP)
CRP is a protein produced by the liver from Interleukin-6. Interleukin-6 is a cytokine both produced when an infection occurs, but also as part of the Senescence Associated Secretory Phenotype (SASP). By taking weekly CRP tests it was possible to identify a background CRP level which when there is no infection indicates the burden of senescent cells.
This was reduced during the citrate supplementation from 0.5 mg/L to under 0.15mg/L (which is the testing threshold of the most sensitive lab test.
This implies an association of citrate supplementation with a reduction in senescence. (see chart).
In the chart it can be seen how an infection from time to time increases IL-6 and CRP, but then it goes back down to the "too low to measure" value.
It should be noted that 0.15mg/L is a very low value for CRP for an older human male.
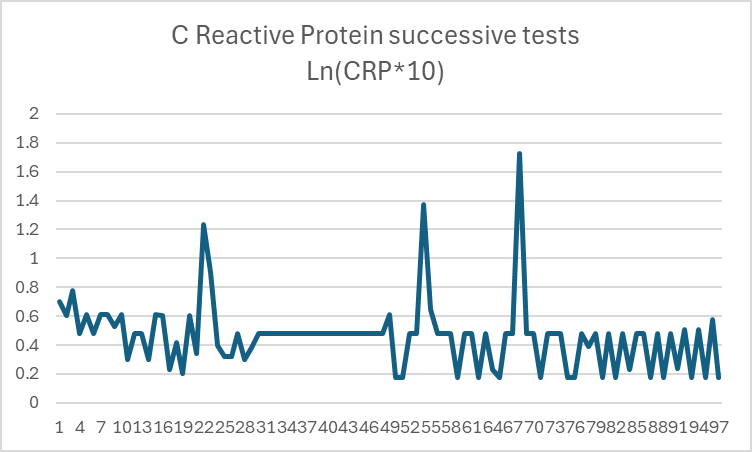
Notes on the chart: The chart uses the natural logarithm of the value of CRP in milligrams per litre multiplied by 10 for successive measurements of CRP. The natural logarithm is used because the high values are many multiples of the low values. One value was excluded because it appears the lab tested someone else's sample. The value is multiplied by 10 because it otherwise would provide a negative logarithm. The minimum values dominate at 0.3 and 0.15 for two labs, but the principle of infection driving the value high and then it falling back is clear.
Inflammatory Markers Change with Age, but do not Fall Beyond Reported Normal Ranges
Some senescent cells are those stuck in the process of differentiation
The author is working on a model of senescence where some senescent cells are stem cells which have failed to differentiate properly as a result of an underexpression of SLC25A1. Interleukin-10 is an inhibitor of NF kappa B which is a transcription factor for SLC25A1. IL-10 is also part of SASP. Hence it is a good candidate for a feedback loop. Interestingly there is some evidence that points to this and that IL-10 can cause senescence.
Decoding the role of IL-10 in aging
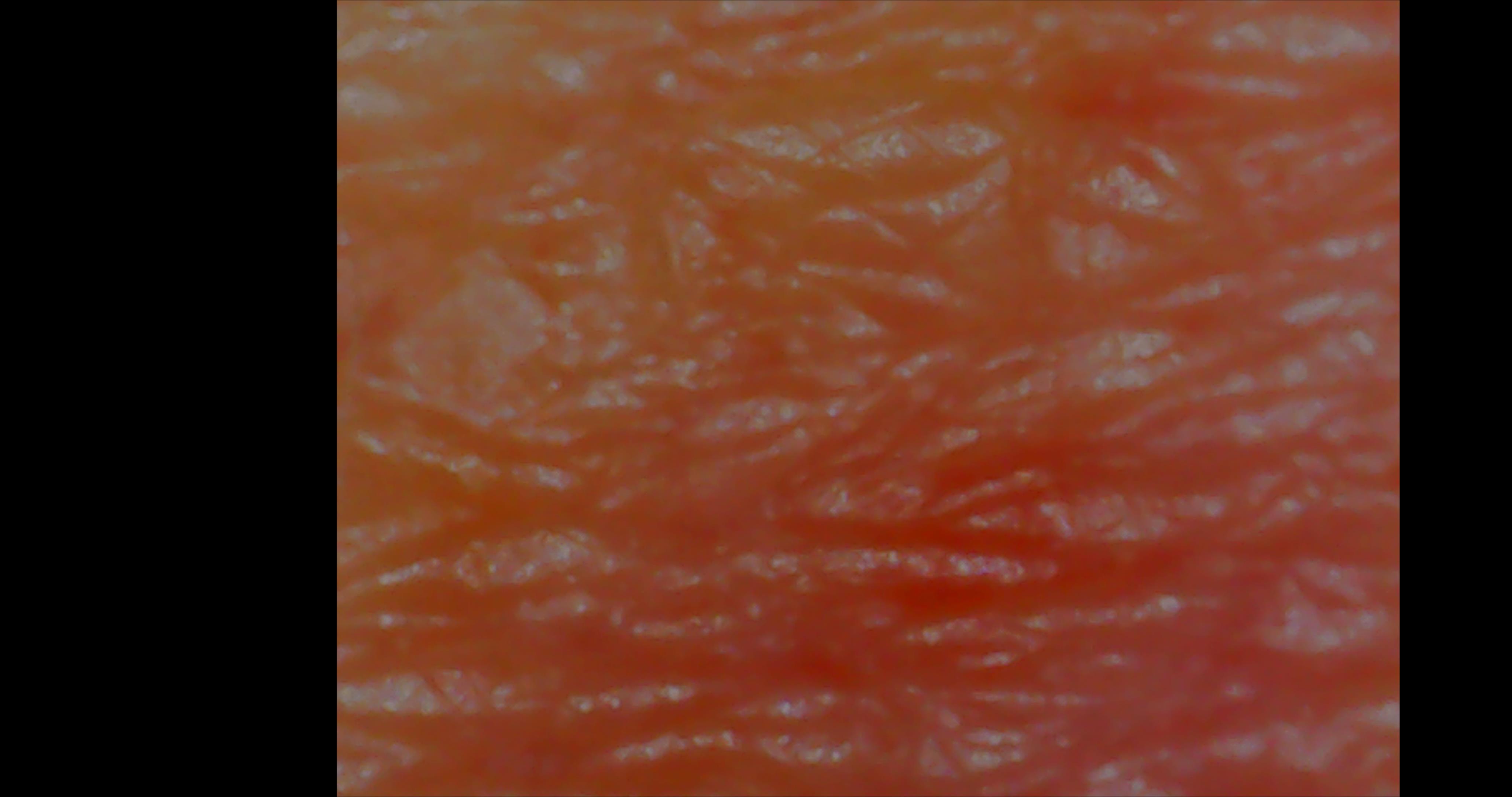
Hair Growth
The test subject has hereditary Male Pattern Baldness. Although he was not entirely bald at the start of the process, he had lost a lot of hair.
Citrate supplementation caused the regrowth of hair and a very very slow advancing of the hairline where it was previously receding. This was dose dependent and has resulted in vellus hairs becoming terminal. Interestingly some hairs have changed from being white to pigmented although this is quite rare and the test subject now has a big white bushy beard with pigmented bits rather than a pigmented beard.

In this a small number of hairs can be seen changning from vellus to terminal. A range of new hairs can be seen of varying shaft diameter.
This was a facial hair that started white and then went pigmented.
Muscle Growth and balance
The test subject improved his score on the sitting rising test from 3 to 1. (A lower score is better). Also managed to do chinups (which he has not previously been able to do).
Sitting Rising Test Wikipedia
Geriatric muscle stem cells switch reversible quiescence into senescence
Other phenotypic changes
A number of subjective phenotypic changes have occurred. These are not only as a result of citrate supplementation, but do arise from the wider protocol of which citrate supplementation is an important part. Here are some photos.


Accelerated repair
Having weekly blood tests means that every week an insult occurs to the approximately the same location on a vein on the experimenter's right arm. As the consumption of citrate is varied so does the speed of repair of the venepuncture. To have the most rapid repair of the venepuncture requires citrate supplementation both on the day before the venepuncture, but also immediately after the venepuncture. That accelerates repair and reduces bruising. The figures used are 10g of citrate before the venepuncture and 5g immediately afterwards.
More research on this issue is needed to identify optimum strategies.
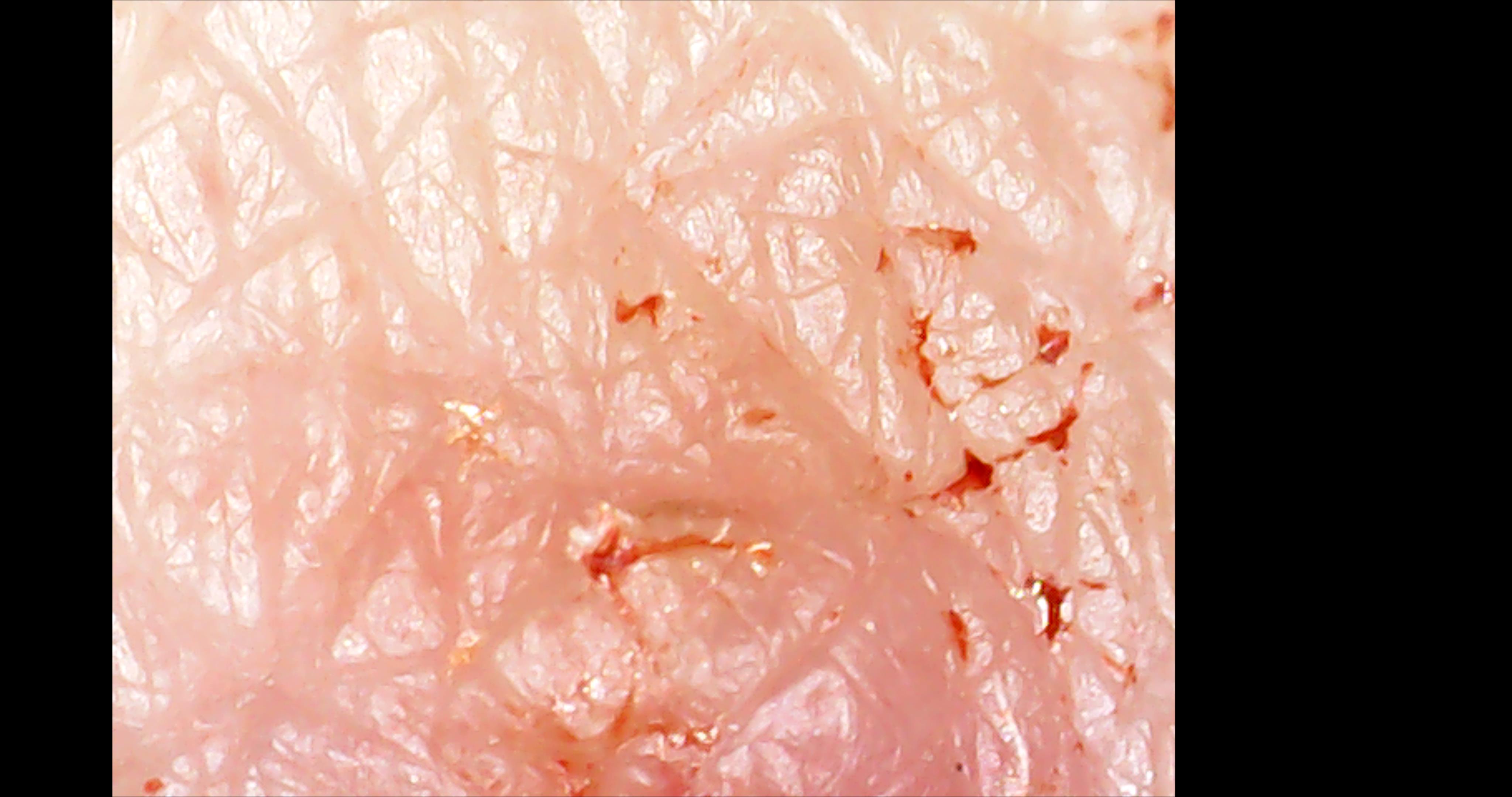
Images of venepuncture repairing in less than 24 hours with citrate supplementation beforehand and afterwards. (Over 10g per day)

Image of venepuncture (from 26/7/24) not repairing in three days without citrate supplementation before the venepuncture, but with citrate supplementation post venepuncture. Without any citrate supplementation it repairs much slower and suffers from substantially more bruising.

Image of having a further venepuncture on 31/7/24 at 10.25am. The previous venepuncture was 26/7/24 at 13.40pm and the insult was visible.

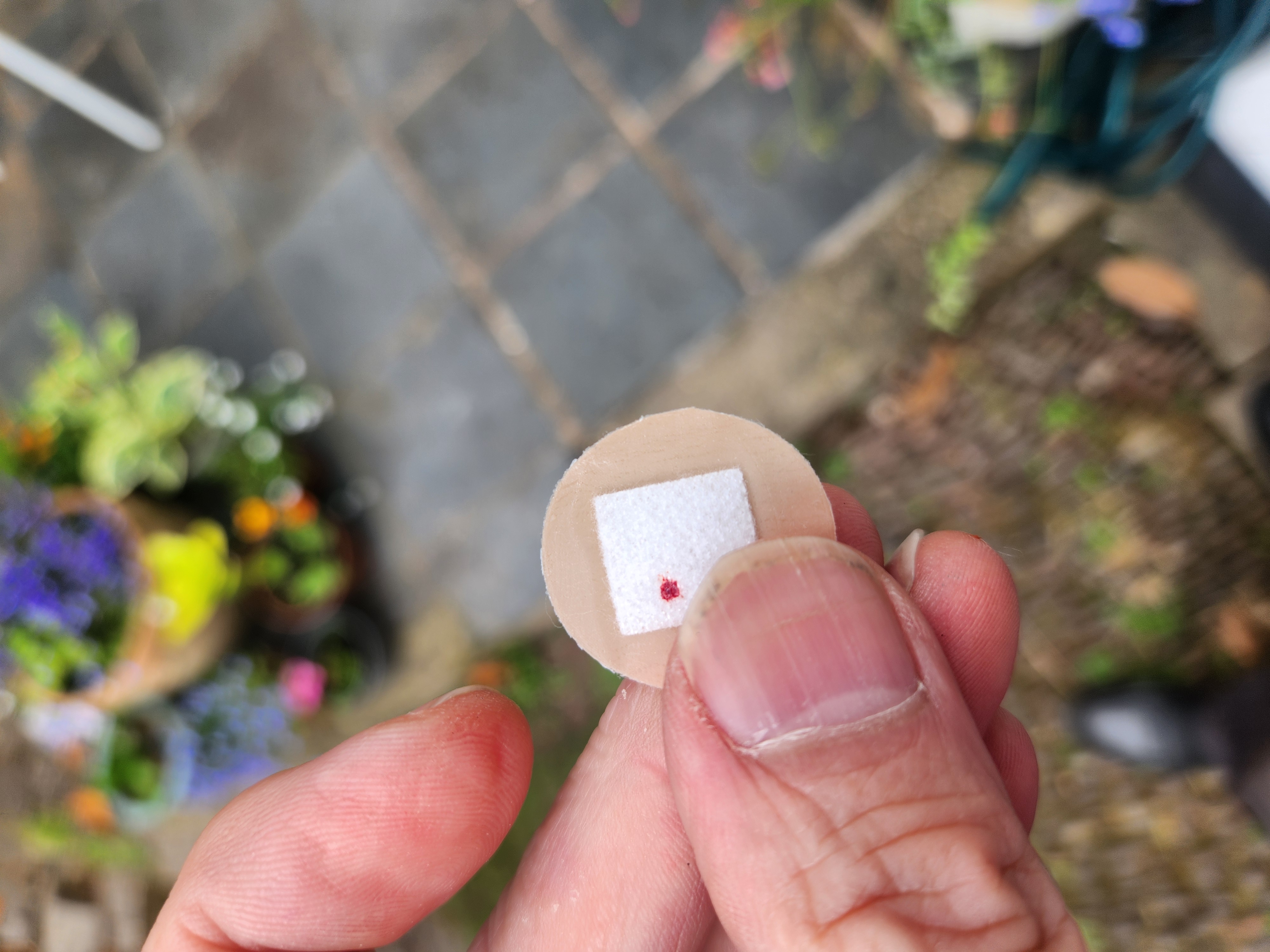
A minute after the venepuncture, it is possible to see both insults. The one from 26/7 which had no citrate supplementation beforehand and the one from 31/7/24 which has caught immediately and not bled and had 15g of citrate supplementation in the day beforehand.

Initially a plaster was placed over the injury, but at 11.45am (one hour and 2 mins after the insult) the plaster was removed and a photo taken. In this photo the insult from 26/7 remains visible and that from 31/7 is now less visible than that of 26/7.

At 6.35 on 1st August the insult from 26/7 is clearly visible, the one from 31/7 (less than 24 hours) is still slightly inflamed, but clearly on its way to full repair. Bilirubin from 26/7 has now gone, but there is none from 31/7.

The next week before the blood tests on 7/8/24 you can see the injury from 24/7, but not the one from 31/7.

Blood is drawn in the same way at 10.30am on 7/8/24.

It looks like it has caught again.

However, you can see through the plaster and it did bleed.
Having removed the plaster you can see the blood on the plaster.

One hour 20 mins after the venepuncture you can see a little blood remaining after the bleed.

However, in the evening less than 12 hours after the venepuncture it is well on its way to repair.

And the next morning less than 24 hours after the venepuncture, the injury from 24/7 remains visible, but that from 7/8 is well on its way to being as well repaired as 31/7 which has not been visible for a number of days.
Renal issues
The biggest challenge with citrate supplementation is the renal clearance of cations. As citrate supplemention is increased with the citrate anion there is a need to also supplement with additional cations. The effect of this on renal markers has been noted. The optimal results for creatinine were as low as 62 micromoles, but it has gone as high as 121. Some of the higher value, however, arose from testing delay causing the sample to metabolise. With Cystatin-C the range is between 0.67 and 1.2 micrograms per litre.
It is important for anyone supplementing with citrate in any substantial amounts (over 5g per day) to monitor renal markers and manage overall kidney demand (also from diet, not just supplementation).
Citrate Toxicity
Citrate Toxicity is a known issue. It arises particularly when patients with hepatic insufficiency receive continuous renal replacement therapy with (normally Sodium) citrate being used for anti-coagulation. Clearly there
is a potential risk with citrate supplementation. Normal dietary citrate levels are thought to be around 4g per day. Experimentation has tended to use 5g in half an hour. Citrate has a molecular weight of 189.1g. Hence if
5g of oral citrate is absorbed entirely by the digestion system that would be 26 millimoles. If it is assumed that it is evenly spread between the 11 litres of extra cellular fluid volume, that would leave 7.2 millimoles in the 3 litres of plasma. That is about 1.6 millimoles in each of the 4.5 litres of blood. This is around
the recommended 1.5 mmol/L level for renal patients although higher concentrations are used. A few post supplementation measurements have been made which found that blood levels were around 0.2 millimoles. However, this probably
did not properly measure the peak. Hence in a person with normal liver function 5g is unlikely to get close to citrate toxicity. However, people with hepatic insufficiency should be careful. More research is needed into
the proportion of citrate that is absorbed into circulation and the relationship between supplementation and serum citrate levels. Clearly there is a sweet spot below toxicity levels, but above normal serum levels at which cytosolic levels
are sufficient to have a beneficial effect, but there is no risk of citrate toxicity.
Let's stop talking about "citrate toxicity"
Construction and validation of a prediction model for the risk of citrate accumulation in patients with hepatic insufficiency receiving continuous renal replacement therapy with citrate anticoagulation
Lithium
Lithium inhibits citrate transporters. Hence care should be taken if supplementing with lithium to ensure sufficient lithium is taken for its longevity benefits, but not so much as to inhibit the citrate transporters. The author hypothesises that the nephrotoxicity of lithium arises from the inhibition of SLC13A2 and SLC13A3 in the kidney.
Molecular properties of the SLC13 family of dicarboxylate and sulfate transporters
Other points of concern
Any experimentation with Citrate at a high level in human beings should be done with care. The increase in cytosolic acetyl-CoA results in a potential increase in cytosolic ROS. This could be useful for dealing with localised infections, but if it is done rapidly in a body with many infections that were previously ignored by the immune system then there could be an increase in localised inflammation. Hence any introduction of citrate supplementation should be done with doses increased gradually. The author also supplements with melatonin which he takes to reduce the impact of ROS and RNS. Clearly also ATP limits will have an effect and increasing transcription rates can go too far.
Methods
A mixture of citrate salts with a range of cations was used (Na/K/Mg/Ca). The quantity of citrate supplemented on a daily basis ranged between 2g and 70g. Because the half life of citrate in serum is around 30 minutes supplementation was normally spread out during the day in order to maintain a higher serum citrate level than is the normal level rather than a high peak that simply decays rapidly. A large range of other interventions was used, but as part of the primary intervention four HDAC inhibitors, curcumin, pterostilbene, quercetin and berberine were used. Additionally Coenzyme A precursor Vitamin B5 and vitamins B9 and B12 were supplemented. These, of course, are not the only inputs. However, they are the inputs directly relevant to mRNA transcription.
Blood was drawn weekly and tested with a range of different laboratories (primarily Randox, Medichecks, NWP, MPS, London Medical). There is some variation between different analyzers and by using a number of laboratories it becomes possible to identify patterns of variation caused by the labs rather than the underlying biomarkers varying.
Debugging the metabolism
The experimental technique of using a large number of interventions and varying them either individually or jointly and measuring any changes has been used. This is the technique used normally for debugging a computer system. It enables a complex system with a number of inputs to be monitored.
Although the process is not placebo controlled or randomised the conclusions give an opportunity for other researchers to test replicabilility. It is, however, recommended that anyone trying this links with the author as the issue of cation clearance is complex. It is possible to have a high level of cations with good kidney biomarkers, but not that straightforward.
Conflicts of interest
The author has made patent applications in connection with his discoveries.
About the author
Born 1960
Educated: King Edwards School, Birmingham.
Scholarship to Magdalen College (Oxford), MA (Oxon) in Physics.
Formed his first business in 1983 which was sold in 2019
Councillor on Birmingham City Council 1990-2008
Deputy Leader of Birmingham City Council 2004-2005
Member of Parliament Birmingham, Yardley 2005-2015
Has been drummer in a heavy metal and punk band in the 1970s then moved into prog rock as a drummer, but more recently is the keyboard player in "John Hemming and the Jazz Lobbyists" which is a well known participant in the Birmingham Jazz Festival.
Leading the XPRIZE Healthspan team "Biohacking to improve everyone's health".
Contact Email: john@hemming.email